
Thursday, October 05, 2006
Demystifying PICU, part 1: Ventilator, Schmentilator
I often hear with some frustration the press talk about patients being in such-and-such a hospital, "on life support".It's a dramatic phrase, but what does it mean? Just about everything we do in critical care can be thought of as life support. Give an adrenaline infusion to keep the heart pumping and the blood pressure at acceptable levels. Insert a drain into the brain's ventricles to prevent pressure from building up and killing the patient. Use a baby warmer or incubator to prevent hypothermia. All of it is life support.
What the press really mean, at least most of the time, is that the patient is on a ventilator. The breathing machine. The bit with the accordion going up and down that you see in the movies (actually, most modern vents don't have those things in 'em but it looks cool, so movies are taking awhile to catch up.)

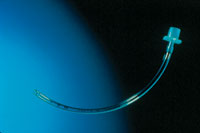
Normally when we breathe we suck air in. We create a slight negative pressure in our lungs which draws in air from the atmosphere. Positive pressure ventilators shove air in, sometimes using quite high pressures, and allow it to flow back out again. Usually the air is pushed in via an endotracheal tube, or ETT inserted through the nose or mouth and down the windpipe.
This is not a natural way for a person to breathe. There are long-term consequences of this kind of treatment on the lungs, which are worse depending on the pressure and volume of gas used. The lungs can become scarred and inflexible, occasionally even punctured. Infections can develop. The entire process is highly stressful for both patient and family.
It's a regular activity for me to have to stop a person from breathing. Sound crazy? Sometimes we have to take over altogether, so we give a drug which prevents a patient from using most of the muscles in their body, including the diaphragm. I can do this because I know that the settings I put on the ventilator will do the breathing for the patient.
When you think about it, it's a big responsibility. If I screw up, the patient will stop breathing. If I don't take immediate action, they die. I laugh when I hear people talk about nurses 'getting back to basics' which, if you inquire further, is usually thought to involve wiping bottoms and feeding patients. I find it funny because of course I do those things too, but I also perform the slightly more immediate function of preventing children and babies from dying. Not dying eventually, but dying right there and then, in front of me.
That might sound like a grab for attention, and perhaps in a way it is. We deserve it! However, I mention this because I read with depressing regularity articles which misrepresent what nurses actually do. They're often written by people who really should know better. They perpetrate a charming, wistful stereotype of the 'good old days' of nursing with little or no understanding of what the job involves today.
Let me say it plainly: if I am ever unfortunate enough to have a child of mine in hospital on a ventilator, although of course I want a good intensivist involved, my most immediate concern will be to get an experienced PICU nurse at the bedside. Someone who knows the ventilator back to front, all its weaknesses and idiosyncrasies. A nurse who knows exactly what the last blood gas results were, and whether or not her patient was agitated or breathing fast when the test was taken. A nurse who knows what little settings tweak to make when nothing else has worked. I want someone who knows when to leave well enough alone and not fuss over small variations in the blood gas.
Someone who makes me laugh when I think I've forgotten how.
There's a lot of inuendo flying around these days about nurses and what their job should be. Allow me to take this opportunity to remind my readers that most of us are skilled at doing two or more things at once. Yes, even the men! We do the basics, and we do the more advanced stuff too. I like to call it wiping bottoms and kicking ass. How's that for a mixed metaphor?
(Now, if only I can get HK to let me change Mediblogopathy's slogan to, "Wiping bottoms and kicking ass since 2003"...)
Next Friday: Chaos Theory.
Posted by PaedsRN at 5:00 PM















I agree! We've come a long way from the hand-maiden days of doing laundry, boiling instruments, and making coffee.
I think this slogan is more up your alley:
http://www.cafepress.com/sdstoreroom.41536832
;)
-HK
oo, chaos theory! looking forward to it.
I love it, HK! :)